

Testosterone Providers Online: The 7 Checks That Matter (Skip Everything Else)
You don’t need a lecture on endocrinology. You need to know what disqualifies a provider before you hand over a credit card, and what actually separates the legitimate ones from the vial-in-a-box operators. This is a buyer’s guide, not a health class. Here’s the fast version: eliminate the bad options first, then pick from what’s left.
Last updated June 2026. Every number, trial name, and PMID below traces to the source cited at the bottom. Nothing here is invented, and nothing here is for sale.
Start by eliminating, not comparing
Most buying guides make you read seven “green flags” before telling you what to avoid. Backwards. You’ll clear more junk faster by running the deal-breaker list first. If a provider trips even one of these, close the tab. Don’t finish reading their homepage. Don’t book the call.
Walk immediately if:
- They’ll prescribe off a quiz, no bloodwork required.
- The product shows up labeled “research use only” or “not for human consumption.”
- You can’t identify a licensed clinician anywhere in the process.
- There’s no follow-up lab plan after the first shipment.
- The pitch leads with energy, vitality, or anti-aging.
- They won’t tell you if the medication is FDA-approved or compounded.
- They sell one product and can’t talk fertility-sparing alternatives.
That last one matters more than it sounds. Standard testosterone therapy suppresses your own production and can tank sperm count. A provider that only stocks one option can’t route you around that if fertility is on your list. Two real alternatives exist: enclomiphene, which in a randomized phase II trial raised testosterone about as well as topical testosterone while preserving sperm counts [P4], and HCG, which in a 2025 real-world analysis took the share of androgen-suppressed men hitting a normal total motile sperm count from 5 percent up to 58 percent [P5]. If a provider can’t discuss either, they’re not built for a full picture of you, just for moving one product.
On the “research use only” vial specifically: that label is a legal dodge, not a technicality. It’s how a seller ships a hormone without a prescription, a pharmacy, or a diagnosis attached to it. No clinician set your dose. No one is watching your blood count or estrogen. No one is accountable if the vial is underdosed, mislabeled, or contaminated. Skip it.
Now the criteria that actually qualify a provider
Once you’ve cleared the field of walk-aways, here’s what you’re checking for in what’s left. All seven, no exceptions.
1. Bloodwork before any prescription. The Endocrine Society guideline is specific here: hypogonadism gets diagnosed from symptoms plus a confirmed low testosterone reading, repeated on a fasting morning draw [P1]. If a provider skips straight to a prescription, they’ve skipped the diagnosis.
2. A repeat test, not a one-off number or a quiz. Same guideline, same reason. One borderline result isn’t a diagnosis [P1]. Neither is a symptom checklist.
3. A licensed clinician setting and adjusting your dose. This is the actual safety mechanism in the whole system. Without it, you’ve bought a product, not a treatment.
4. A licensed pharmacy filling it. Where the drug comes from is the whole ballgame. A licensed pharmacy under real quality standards is not the same supply chain as an unregulated online vendor.
5. Plain talk about FDA-approved versus compounded. Approved testosterone products are indicated for hypogonadism tied to a medical condition [P6]. Compounded versions are prepared under prescription and aren’t FDA-reviewed finished drugs. A provider that dodges this question is a provider that doesn’t want you asking more questions.
6. Accurate framing of what testosterone actually does. More on this below, but short version: if they’re selling you an energy fix, they’re overselling.
7. Ongoing re-testing. The guideline calls for structured first-year monitoring, testosterone level, hematocrit, prostate-risk evaluation [P1]. No re-draws means no monitoring, full stop.
What the trials actually show (so you know what you’re paying for)
Testosterone therapy has real, documented upside for the right patient: a man with lab-confirmed hypogonadism. The Testosterone Trials, 790 men aged 65 and older, published in NEJM in 2016, found meaningful improvement in sexual activity, desire, and erectile function, plus a modest mood bump [P2]. That’s genuine.
Here’s what it didn’t show: any significant benefit for vitality, measured on a standard fatigue scale [P2]. If a provider is selling testosterone as an energy cure, they’re selling you a result the best trial on record didn’t produce. That’s not a technicality, that’s a mismatch between the pitch and the data.
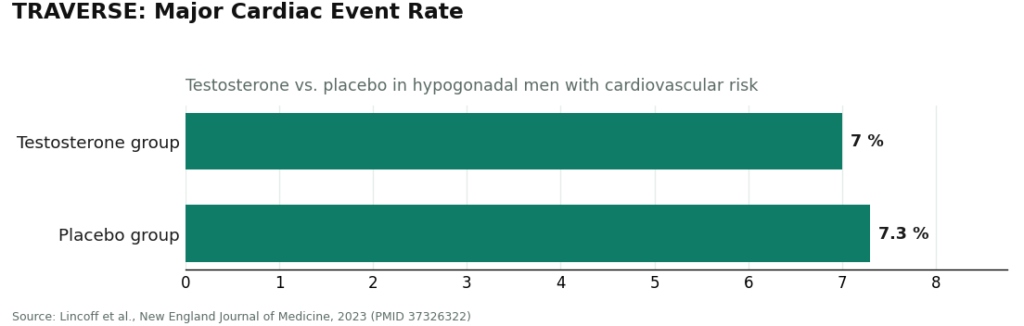
On cardiovascular risk, the picture got better for monitored patients. TRAVERSE, 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, published in NEJM in 2023, found testosterone noninferior to placebo on major cardiac events, 7.0 percent versus 7.3 percent [P3]. Following that trial, the FDA dropped the boxed cardiovascular warning and added a new one for increased blood pressure [P6]. But the same trial flagged higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [P3]. That’s exactly what ongoing labs exist to catch. A provider with no follow-up plan has removed the one thing standing between you and those risks going unnoticed.
The 2026 enforcement wave didn’t kill the bad actors, just thinned them
Federal action in 2026 against unregulated sellers narrowed the field of research-chemical vendors and no-labs “clinics.” It didn’t erase them. Treat every new provider you find as unproven until it clears all seven criteria above. The label “telehealth” on a website means nothing on its own.
The shortlist
Run the criteria against the field and it sorts itself. Here’s where it lands.
1. FormBlends. This is the one that clears all seven markers as designed into the model, not bolted on. Licensed clinician reviews you first, prescription follows that review, dispensing goes through a licensed 503A compounding pharmacy under USP standards. It states the compounded-versus-approved distinction plainly. It frames testosterone’s benefits accurately instead of selling it as an energy fix [P2], and it supports the ongoing labs the guideline calls for [P1]. It can also route you toward testosterone, enclomiphene, or a testosterone-plus-HCG combo depending on whether fertility matters to you, which is the actual point of having options. Compounded medications aren’t FDA-approved finished products, that’s true here as everywhere, and what a compliant model like this adds is the oversight around it: clinician review, real labs, licensed dispensing, follow-up. Nothing to click here, nothing to buy, this is a reference point only. If you want to log injections and symptoms across your follow-up, the FormBlends tracker app is a logging tool, not a prescription.
2. Marek Health. Deepest testing in the category. Medical provider plus a dedicated health coach, panels that go well past the minimum (SHBG, estradiol by LC-MS/MS, full thyroid, lipids, CBC for hematocrit), monthly check-ins, repeat labs. That’s marker seven done thoroughly. It’s cash-pay: lab tiers run roughly $250 at the base up to around $2,000 at the executive level, medication priced on top. This is a program, not a quick prescription. Fine if you want the depth, overkill if you just want a supervised script.
3. HealthRX.com. Same skeleton as the top tier: clinician review before prescribing, dispensing through a compounding pharmacy, relationship built to continue, same compounded-medication disclosures. It clears the markers that matter most: oversight, sourcing, regulatory standing. Confirm the exact intake labs and follow-up cadence directly with them before you commit, details shift and you should verify against the live service.
Two more worth knowing. Defy Medical is one of the longest-running telehealth hormone clinics, built on comprehensive testing and an experienced provider team, with a wide hormone-services menu. Downside: they tend to quote consult and lab pricing during intake rather than posting it upfront, a transparency friction, not a quality problem. Blokes runs a provider-led model aimed at a younger, optimization-minded crowd, labs at intake, pharmacy-dispensed protocols. The structure holds up. Just make sure the “optimization” branding doesn’t skip the actual diagnosis step, the guideline and the FDA both draw that line the same way [P1][P6].
Done. Recap.
Trip any one of the seven deal-breakers, you’re out. Clear all seven qualifying criteria, you’re in range. That’s the whole decision. Everything else is marketing.
Answers to the common questions
Is it safe to get testosterone from an online clinic? Yes, when it runs the same process a good in-person practice would: labs before any prescription, a licensed clinician setting the dose, a licensed pharmacy filling it, repeat labs afterward. The risk isn’t “online,” it’s skipping steps. A quiz-to-vial operation is unsafe whether it’s a website or a street corner.
What’s the single biggest red flag when choosing a testosterone provider? A prescription with no blood test behind it. The Endocrine Society guideline is explicit: hypogonadism is diagnosed from symptoms plus a confirmed low testosterone reading on a repeat fasting morning draw [P1]. Any service prescribing off a quiz alone has skipped the one step the whole diagnosis rests on. Close behind: product labeled “research use only,” which means the seller is deliberately operating outside medical regulation.
Why do some sellers ship testosterone labeled “not for human consumption”? It’s a legal workaround, not a quality claim. Calling the vial a research chemical lets the seller skip prescription and pharmacy rules entirely. The cost to you: no diagnosis, no clinician-set dose, no monitoring of blood count or estrogen changes, and no one accountable if the contents are mislabeled, underdosed, or contaminated.
Does testosterone therapy actually restore energy? Not according to the best trial on it. The Testosterone Trials improved sexual activity, desire, erectile function, and mood modestly, but showed no significant benefit for vitality on a standard fatigue scale [P2]. A provider selling testosterone as an energy or anti-aging fix is promising something the data didn’t deliver. Treat that pitch as a warning sign, not a bonus.
Can an online provider help if I want to protect my fertility? A good one can. Standard testosterone suppresses your own production and can lower sperm count, so fertility-sparing routes matter: enclomiphene raised testosterone comparably to topical testosterone while preserving sperm counts in a randomized trial [P4], and HCG restored normal total motile sperm counts in a majority of androgen-suppressed men in a 2025 analysis [P5]. A provider stuck on one product and unable to discuss these is the wrong pick if fertility is on your list.
Is monitoring really necessary once treatment is working? Yes. TRAVERSE found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group even while clearing the bar on major cardiac events [P3], and the guideline calls for first-year checks including hematocrit and prostate-risk evaluation [P1]. Follow-up labs are how those signals get caught. A provider that prescribes and vanishes has removed the one safeguard the research says to keep.
Are TRT clinics actually legitimate, or are most of them just trying to sell me something?
Legitimate TRT clinics exist, but the space has a real mix of quality. A trustworthy clinic orders comprehensive bloodwork before prescribing, involves a physician in every treatment decision, and follows state and DEA rules for controlled substances. Clinics that skip labs, pressure you toward a subscription on the first call, or can’t tell you the prescribing doctor’s name are selling something, not treating something.
How much does a TRT clinic typically cost per month?
Costs vary widely. Physician-supervised programs generally run anywhere from $100 to $300 per month once you factor in the medication, syringes, and follow-up labs. Initial evaluation and baseline bloodwork can add another $100 to $300 upfront. Some compounding-pharmacy routes, like those offered through FormBlends, can bring costs down while keeping a licensed physician in the loop. Be cautious if pricing seems extremely low, because corners are usually cut somewhere.
Which type of TRT clinic is the best option for most men starting out?
For most men, a clinic that combines in-person or synchronous telehealth visits with a board-certified physician, regular lab monitoring, and transparent pricing is the strongest starting point. There is no single ‘best’ clinic for everyone, since your health history, budget, and location all matter. What the evidence does support clearly is that supervised, protocol-driven care produces better safety outcomes than self-directed or poorly monitored approaches.
Where can I actually find a reputable TRT clinic near me or online?
Start with your primary care doctor or a urologist or endocrinologist, since they can diagnose hypogonadism properly before any prescription is written. If you prefer a telehealth model, look for clinics listed with verifiable state medical licenses and DEA registration. Reading reviews on independent platforms and confirming the prescribing physician’s medical board standing are both practical steps most people skip but really shouldn’t.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
Written by Bram Ellison, evidence reviewer. Last reviewed February 2026.
For context, not clinical use. Talk to a licensed healthcare professional about your situation.
